
Hematological High-Risk Care
Safeguarding Your Baby in an Rh-Negative Pregnancy.
Being Rh-Negative is simply a blood type, but it requires highly specialized monitoring during pregnancy. Dr. Kunda Shahane provides the non-invasive MCA Doppler imaging and elite interventions needed to protect your baby from fetal anemia and ensure a healthy delivery.
Schedule Fetal AssessmentYour Blood Type is Not a Barrier to a Healthy Baby.
When a mother discovers she has an Rh-Negative blood type (like O-, A-, B-, or AB-), she often reads frightening information online about her immune system "attacking" the baby. It is completely natural to feel anxious, but we want to reassure you: With proper medical surveillance, Rh incompatibility is highly predictable and deeply manageable.
The concern only arises if your baby inherits an Rh-Positive blood type from their father. If a tiny amount of the baby’s blood crosses into your bloodstream, your body may recognize it as foreign and create antibodies. This process is called Alloimmunization (or Isoimmunization). While your general obstetrician manages preventative care, a Fetal Medicine Specialist steps in to monitor the baby directly if those antibodies begin to affect the pregnancy.
The Risks We Actively Prevent
If maternal antibodies cross the placenta, they target the baby's red blood cells. We monitor for these specific complications.
Fetal Anemia
As maternal antibodies break down the baby's red blood cells, the baby can become anemic. Severe anemia means the baby struggles to get enough oxygen to their vital organs. Early detection through our advanced ultrasound protocols is absolutely critical.
Fetal Heart Strain
When a baby is anemic, their heart has to pump significantly harder and faster to try and circulate the limited oxygen available. Over time, this extreme exertion can lead to cardiac stress, which we monitor via Fetal Echocardiography.
Hydrops Fetalis
If fetal anemia is left undetected and untreated, the baby's heart can begin to fail, causing abnormal fluid to build up in their chest, abdomen, or under their skin (hydrops). Our entire Fetal Medicine protocol is designed to intervene long before this severe stage occurs.
Neonatal Jaundice
The breakdown of red blood cells produces a yellow substance called bilirubin. While the placenta clears this during pregnancy, the baby may experience severe jaundice immediately after birth, requiring coordinated care with our neonatology team.
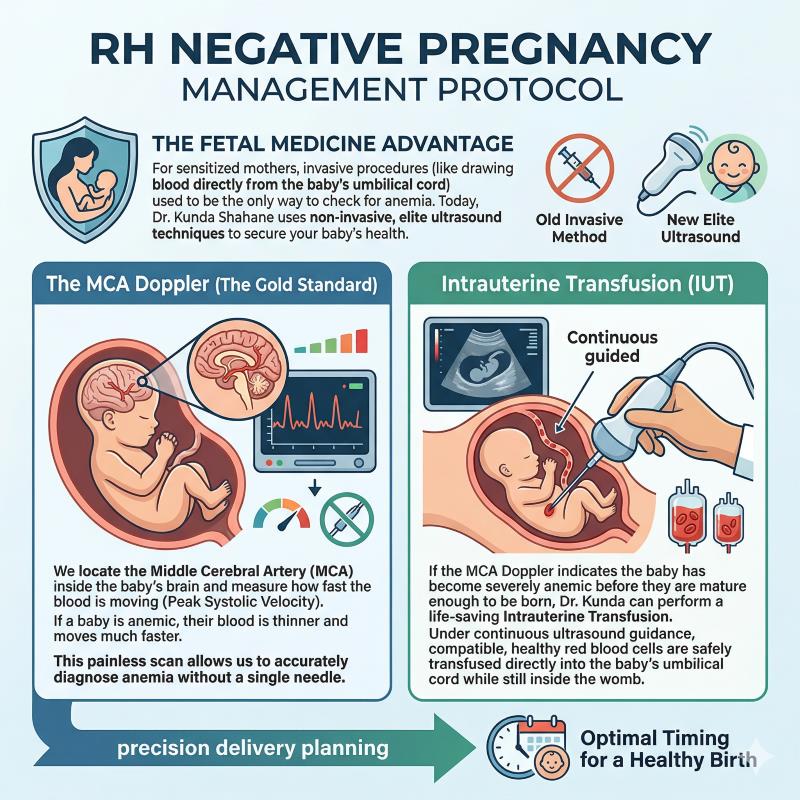
The Fetal Medicine Advantage
For sensitized mothers, invasive procedures (like drawing blood directly from the baby's umbilical cord) used to be the only way to check for anemia. Today, Dr. Kunda Shahane uses non-invasive, elite ultrasound techniques to secure your baby's health.
The MCA Doppler (The Gold Standard)
We locate the Middle Cerebral Artery (MCA) inside the baby's brain and measure how fast the blood is moving (Peak Systolic Velocity). If a baby is anemic, their blood is thinner and moves much faster. This painless scan allows us to accurately diagnose anemia without a single needle.
Intrauterine Transfusion (IUT)
If the MCA Doppler indicates the baby has become severely anemic before they are mature enough to be born, Dr. Kunda can perform a life-saving Intrauterine Transfusion. Under continuous ultrasound guidance, compatible, healthy red blood cells are safely transfused directly into the baby's umbilical cord while still inside the womb.
Precision Delivery Planning
By mapping the precise trajectory of the baby's health week by week, we work with your primary Obstetrician to perfectly balance the risks of early delivery against the risks of keeping the baby in the womb, ensuring the safest possible birth day.